




You’ve likely heard the exciting news that CooperVision has received U.S. Food and Drug Administration (FDA) approval of its MiSight® 1 day contact lens[1], indicated to slow the progression of myopia (nearsightedness or short-sightedness) in children, aged 8-12 at the initiation of treatment.
What you may not know that CooperVision has been involved with myopia research for the past 15 years. One significant area of interest is understanding potential risks of interventions to manage myopia vs. the potential benefits that these interventions can give to patients. Dr. Mark Bullimore MCOptom, PhD, FAAO, is a clinical scientist whose many research interests include myopia and children’s vision. Dr. Bullimore shared his retrospective analysis of prior studies on risks of vision impairment from myopia and complications arising from contact lens wear at the American Academy of Optometry in Orlando, Florida.[2]
Dr. Bullimore performed this retrospective analysis because myopia management has the potential to reduce the risk of visual impairment later in life by lowering a patient’s ultimate level of myopia, but this benefit has not been quantified, nor has it been compared with the potential risks of visual impairment associated with myopia management modalities. This work is the first to quantify potential benefits of myopia management using the data for visual impairment as a function of myopia from Tideman et al.[3] and Bullimore et. al.[4], and the risk of visual impairment associated with different contact lens modalities using data from Stapleton[5] et al. and Bullimore et. al.[6].
From a contact lens wearing safety perspective, a large study performed by Stapleton et. al. found that daily disposable contact lens wear had the lowest risk of microbial keratitis (MK) with less than 2 incidents of MK per 10,000 patient years of wear.5 Regular overnight wear represented the largest risk of (MK) with 25 cases per 10,000 patient years of wear. A subsequent analysis specific to studies that focused on studies of contact lens wear by children by Dr. Bullimore found that the incidence of corneal infilitrative events were much lower in young children than in adults.6 Furthermore, there were no reported cases of MK in over 2400 patient years of contact lens wear. Data from the contact lens assessment in youth (CLAY) study7 also shows a low rate of ocular incidents with contact lens wear in younger children (Figure 1).
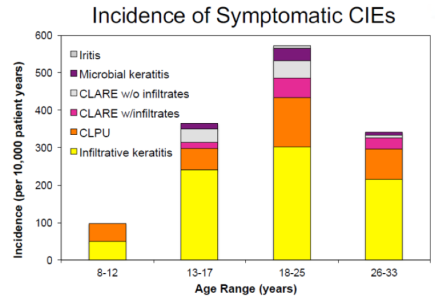
Figure 1. Incidence of Symptomatic Corneal Infiltrative Events (CIEs) with contact lens wear in various age ranges.[7]
So now that we’ve gotten a handle on the relatively small level of risk involved in young children wearing contact lenses, what about the benefits of myopia management? The potential benefits are significant. A recent paper by Dr. Bullimore and Dr. Brennan quantified the potential benefits of lowering myopia by just a diopter.4 They found that slowing myopia by 1 diopter should reduce the likelihood of a patient developing myopic maculopathy by 40% and vision impairment by 20%.
This presentation at the recent Academy meeting2 specifically compared the years of uncorrectable visual impairment that might be prevented by lowering patients’ ultimate level of myopia by 1 D (over the 70 years average remaining lifespan) with the corresponding years of visual impairment associated with 5-years of contact lens wear (the average myopia management treatment period). From this analysis it was found that myopia management (assuming a reduction in myopia progression of 1D) could potentially prevent 5,000 – 10,000 years of potential vison loss per 10,000 patient years while the years of potential vision loss that could occur via a 5 year myopia management intervention with daily wear soft contact lenses is between 53-106 years of potential vision loss per 10,000 patient years. From these calculations the analysis concludes that the benefits of myopia control significantly outweigh the risks associated with daily wear of contact lenses in children.
So what does all this mean for your practice?
In the United States, children younger than 10 years old are less likely to be fitted in contact lenses.[8] However, the AOA recommends that myopia correction and control measures should begin early in life because early-onset myopia is associated with more rapid progression and eventual development of high myopia, which increases the risk of retinal detachment, cataracts, glaucoma, and other conditions.[9] Therefore, a natural question from parents when a myopia management strategy is proposed may be around the risks of myopia management vs. the benefits. The presentation summarized above and the studies cited in this article may be helpful resources for parents to better support the conversation about the relative risks and possible benefits of myopia management with soft contact lenses, such as MiSight®1.
To learn more about pediatric myopia and to sign up to receive updates about MiSight® commercial availability in the U.S., go to https://coopervision.com/practitioner/myopia-management
To read Dr. Bullimore’s peer-reviewed, open-access, publication on the safety of contact lens wear in children go to:
https://journals.lww.com/optvissci/toc/2017/06000
[1] MiSight™ (omafilcon A) daily wear single use Soft Contact Lenses are indicated for the correction of myopic ametropia and for slowing the progression of myopia in children with non-diseased eyes, who at the initiation of treatment are 8-12 years of age and have a refraction of -0.75 to -4.00 diopters (spherical equivalent) with ≤ 0.75 diopters of astigmatism. The lens is to be discarded after each removal.
[2] “Myopia Control: An Evidence-Based Comparison of the Benefits and the Risks”. M. Bulllimore, E. R. Ritchey. Fall 2019 American Academy of Optometry National Meeting.
[3] Tideman, J. W. L. “Association of Axial Length with Risk of Uncorrectable Vision Impairment for Europeans with Myopia.” JAMA Opthamol., 134(12), 1355-1363.
[4] Bullimore, M.; Brennan, N. “Myopia Control: Why Each Diopter Matters.” Optom Vis Sci. 2019 Jun;96(6):463-465.
[5] Stapleton, F. et. al. “The Incidence of Contact-Lens Related Microbial Keratitis in Australia.” Ophthalmology, 115, 1655-1662.
[6] Bullimore, M. “The Safety of Soft Contact Lenses in Children” Optometry and Vision Science: June 2017 - Volume 94 - Issue 6 - p 638–646
[7] Chalmers et. al. “Age and Other Risk Factors for Corneal Infiltrative and Inflammatory Events in Young Soft Contact Lens Wearers from the Contact Lens Assessment in Youth (CLAY) Study”. Invest. Ophthalmol. Vis. Sci., 2011, 52, 6690-6696.


